Brachytherapy is a form of treatment for prostate cancer, where radioactive seeds of iodine 125 (I125) are placed permanently in the prostate gland. The term “Brachytherapy” was chosen because in ancient Greek “brachy” means “short”, which indicates that the radioactivity is administered directly to the cancerous tissue. This is in contrast with traditional external beam radiation, where the radioactivity unavoidably passes through healthy tissue before reaching the prostate. Brachytherapy delivers higher and more localized radiation to the prostate, while minimizing the effect on the neighbouring organs such as the bladder and rectum.
The radioactive seeds are small “cartridges” of titanium (4.5mm long by 0.8mm diameter) containing the radioactive isotope iodine-125. The half-life (time required for the radioactivity to reduce by half) is about 60 days, which means that most of the radioactivity is released into the prostate during the first three months. The granules remain biologically active for a total of approximately 9 months. After this, they become virtually inactive.
Long-term results from U.S. patients who underwent Brachytherapy over 15 years ago, show that it is a very effective form of treatment for patients with localized prostate cancer.
Brachytherapy compared with other treatments (radical prostatectomy, external radiation) seems equally effective, but has fewer side effects and complications.
However Brachytherapy is not of course the only effective form of treatment for prostate cancer and some patients may have evidence for another form of therapy.
Initial Consultation and Patient Selection
During the first consultation or assessment visit you will see the urologist surgeon responsible for Brachytherapy, Stelios Voulgaris. He will begin with your general medical history, inwhich previous illnesses, surgeries, medications, etc. will be noted.
A digital rectal examination of the prostate will follow to determine the stage of cancer. Then a painless ultrasound will determine the size of the prostate.
You will then be asked to complete a short questionnaire to determine any “voiding” symptoms – thus you will be asked in advance to arrive at your consultation with a relatively full bladder. You will then need to urinate in a special machine (Uroflow System) and have measured by ultrasound any remaining urine in the bladder.
A discussion will follow on the stage and grade of the cancer and whether or not you are a suitable candidate for Brachytherapy.
At the end of this initial consultation, if you are a suitable candidate for Brachytherapy and decide to choose this form of treatment, dates will be discussed for the next stage of the therapy.
Patients suitable for Brachytherapy are those whose cancer still has a high chance of being confined within the prostate, without spreading to the near or distant organs. In some cases, when there are indications that the cancer has spread to a small area in surrounding tissues, the patient may need to receive a treatment of five weeks of external beam radiation therapy prior to Brachytherapy. This combination treats a more extensive tissue area around the prostate.
The Brachytherapy team will advise you whether or not you are a suitable candidate for Brachytherapy. Patients suitable for brachytherapy typically have the following characteristics:
- The PSA (Prostate Specific Antigen) should ideally be less than 20ng/ml at diagnosis.
- The cancer should be at stage T1 or T2 in the digital rectal examination, suggesting limited cancer within the prostate.
- The malignancy Grade should ideally be Gleason Score 7 / 10 or less.
- Patients should not suffer from significant urological symptoms such as decreased range of urination or difficulty emptying the bladder.
- Ideally the prostate should be relatively small – less than 50cc. If the prostate gland is very large, some areas of the gland may be “hidden” behind the pelvis, making it impossible to achieve a satisfactory implant.
Treatment
Brachytherapy for prostate cancer takes part in two stages. Stage one involves a transrectal ultrasound examination of the prostate, while Stage two involves the implantation of the radioactive seeds and can either be done at once (using the “Real-time” technique), or about four weeks later (the “Seattle technique”).
1st Stage – Prostate Examination
This is a detailed ultrasound examination, typically performed as a day case (no hospital stay) under general or local anesthesia – with the patient going home shortly afterwards. As preparation, the patient will receive a laxative beforehand, in order for the bowels to be as empty as possible to allow a reliable sonographic image to be viewed. During the examination, a volume catheter will be inserted into the urethra. The catheter helps to clearly distinguish the urethra during the study. The catheter will be removed immediately after the procedure.
The volume of the prostate and the position of the urethra and rectum are recorded in the prostate examination.
Then, specialist Brachytherapy software creates a 3D model of the prostate and produces a plan for the dosage. This plan is unique to each patient and determines the location and number of radioactive seeds required – these seeds are then ordered.
In some cases, when the volume of the prostate is large (between 50-80cc), treatment with the seeds may need to be preceded by three months’ worth of hormonal therapy to reduce the size of the prostate and thus allow the implantation of radioactive seeds.
2nd Stage – Implantation of seeds
Patients are usually admitted to hospital the day of the treatment. Adequate bowel preparation is necessary here.
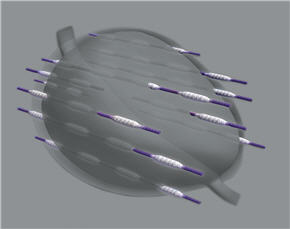
The surgery is performed under general anaesthetic. The implantation of radioactive seeds is done under ultrasound guidance adjusted using a special needle inserted through the perineum. Each needle helps to introduce 2-6 seeds and usually 20-30 needles are used to introduce 80-120 seeds. The granules are attached to an absorbable thread, which ensures that they remain at the site of implantation. The seeds remain at the point of implantation permanently. A urethral catheter is inserted, as in Stage 1 – the only difference being that the patient now remains in hospital until the next morning.
Χρησιμες Πληροφοριες
Ακράτεια Ούρων
Η ακράτεια ούρων μετά απο βραχυθεραπεία προστάτη είναι ένα εξαιρετικά σπάνιο φαινόμενο. Η διεθνής βιβλιογραφία αναφέρει ποσοστό ακράτειας μετά βραχυθεραπεία μικρότερο του 1%.
Στυτική δυσλειτουργία
Οι στύσεις μπορεί να επηρεασθούν με τη βραχυθεραπεία. Η πιθανότητα είναι μικρότερη σε νεότερους ασθενείς, οι οποίοι δεν είχαν προβλήματα στύσεως πριν τη θεραπεία και τείνει να επηρεάζει περίπου 25% των ασθενών μας μετά τη θεραπεία. Πρόσφατες μελέτες έχουν δείξει πως η πιθανότητα στυτικής δυσλειτουργίας είναι μικρότερη συγκρινόμενη με άλλες θεραπείες, όπως η ριζική προστατεκτομή. Η επιπλέον θεραπεία με φάρμακα, όπως το Viagra, είναι συνήθως αποτελεσματική στο 80% των ασθενών με δυσκολίες στην επίτευξη ή διατήρηση ικανοποιητικής στύσης.
Επιστροφή στις καθημερινές δραστηριοτητές
Θα είστε ικανός να επιστρέψετε στις καθημερινές σας δραστηριότητες (εργασία, ψώνια κτλ) εντός ολίγων ημερών. Παρόλα αυτά, συνιστάται η αποφυγή βαρειάς εργασίας ή το σήκωμα βάρους για τις πρώτες δυο εβδομάδες.
Οικογενειακές σχέσεις
Μπορείτε να κοιμάστε στο ίδιο κρεβάτι με τη σύντροφο σας εφόσον δεν είναι έγκυος. Η σεξουαλική επαφή, με τη χρήση προφυλακτικού, μπορεί να αρχίσει ένα μήνα μετά τη θεραπεία αν το επιθυμείτε. Ο λόγος της αρχικής χρήσης προφυλακτικού είναι η πολύ σπάνια περίπτωση κάποιου απο τους κόκκους να «ξεφύγει» στο σπέρμα.
Το σπέρμα σας μπορεί να έχει σκούρο καφέ ή μαύρο χρώμα τον πρώτο καιρό. Αυτό είναι φυσιολογικό και είναι αποτέλεσμα μικρής αιμορραγίας που συνέβη κατά τη θεραπεία. Μετά απο δυο με τρεις εκσπερματώσεις η χρήση του προφυλακτικού δεν είναι πλέον απαραίτητη.
Ακτινοπροστασία
Πολλοί ασθενείς ανησυχούν για το αν οι εμφυτευμένοι κόκκοι ενέχουν κάποιο κίνδυνο έκθεσης σε ραδιενέργεια της οικογένειας τους ή φίλων. Είναι σημαντικό να θυμάστε, πως ενώ οι κόκκοι είναι ραδιενεργοί εσείς δεν είστε.Οι σωματικές σας αππεκρίσεις (ούρα, κόπρανα κτλ) δεν είναι ραδιενεργά. Επίσης δεν υπάρχουν επίσημοι περιορισμοί στις δραστηριότητες σας μετά την επιστροφή σας στο σπίτι. Παρόλα αυτά, προτείνουμε τη λήψη των ακόλουθων μέτρων για τους δυο πρώτους μήνες μετά τη βραχυθεραπεία. Μετά τους δυο αυτούς αρχικούς μήνες τα επίπεδα ραδιενέργειας μειώνονται αισθητά και έτσι μπορείτε να επιστρέψετε στην φυσιολογική σας καθημερινή ζωή.
- Έγκυες (ή πιθανώς έγκυες) γυναίκες δεν πρέπει να κάθονται πολύ κοντά σας (π.χ. στον ίδιο καναπέ ή στο ίδιο κρεβάτι) για περισσότερο απο λίγα λεπτά τη μέρα. Παρόλα αυτά μπορείτε να συνεχίσετε να τις χαιρετάτε ή να τις αγκαλιάζετε όπως ακριβώς θα κάνατε πριν τη θεραπεία και επίσης να κάθεστε μαζί τους για όσο θέλετε στο ίδιο δώματιο.
- Μην αφήνετε παιδιά να κάθονται στην αγκαλιά σας για μεγάλο χρονικό διάστημα. Όπως αναφέρθηκε παραπάνω μπορείτε να τα αγκαλιάζετε για λίγο και να κάθεστε στο ίδιο δωμάτιο μαζί τους απεριόριστα.
- Άλλα ενήλικα μέλη της οικογένειας, φίλοι ή συνάδελφοι δεν κινδυνεύουν οπότε και δεν υπάρχουν περιορισμοί σε χρoνική διάρκεια επαφής ή γενικά σε δραστηριότητες μαζί τους.
Βραχυθεραπευθέντες ασθενείς
Ο ουρολόγος Στέλιος Βούλγαρης (απεικονίζεται αριστερά) είναι επιστημονικός υπεύθυνος του μοναδικού στη Βόρεια Ελλάδα Κέντρου Βραχυθεραπείας Προστάτη. Στην ενότητα αυτή μπορείτε να μάθετε περισσότερα για την πορεία κάποιων απο τους ασθενείς οι οποίοι έχουν υποβληθεί σε βραχυθεραπεία προστάτη απο την ομάδα του κ Βούλγαρη.
